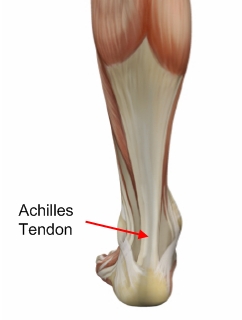
Overview  The Achilles tendon is situated above the heel and forms the lower part of the calf muscles. It is a continuation of the two calf muscles, the gastrocnemius and soleus muscles, and it attaches to the heel bone. It is the strongest tendon in the human body and must withstand great forces. Its function is to transmit the force produced by the calf muscles to lift the heel and produce the push off during walking, running and jumping. The Achilles can produce force of up to seven times body weight. This shows just how much force it has to withstand during sporting activities, such as sprinting, jumping and turning. Causes The causes of an Achilles tendon rupture are very similar to Achilles tendinitis. Causes include. Running uphill. Running on a hard surface. Quickly changing speeds from walking to running. Playing sports that cause you to quickly start and stop. Symptoms Often the person feels a whip-like blow that is followed by weakness in the affected leg - usually he or she is not able to walk afterwards. At place where the tendon ruptured, a significant dent is palpable. Often the experienced physician can diagnose a ruptured Achilles tendon by way of clinical examination and special function tests. Imaging techniques, such as ultrasound and magnetic resonance imaging (MRI) allow for a more precise diagnosis. Diagnosis Your doctor diagnoses the rupture based on symptoms, history of the injury and physical examination. Your doctor will gently squeeze the calf muscles, if the Achilles tendon is intact, there will be flexion movement of the foot, if it is ruptured, there will be no movement observed. Non Surgical Treatment Non-surgical treatment of Achilles tendon rupture is usually reserved for patients who are relatively sedentary or may be at higher risk for complications with surgical intervention (due to other associated medical problems). This involves a period of immobilization, followed by range of motion and strengthening exercises; unfortunately, it is associated with a higher risk of re-rupture of the tendon, and possibly a less optimal functional outcome.
The Achilles tendon is situated above the heel and forms the lower part of the calf muscles. It is a continuation of the two calf muscles, the gastrocnemius and soleus muscles, and it attaches to the heel bone. It is the strongest tendon in the human body and must withstand great forces. Its function is to transmit the force produced by the calf muscles to lift the heel and produce the push off during walking, running and jumping. The Achilles can produce force of up to seven times body weight. This shows just how much force it has to withstand during sporting activities, such as sprinting, jumping and turning. Causes The causes of an Achilles tendon rupture are very similar to Achilles tendinitis. Causes include. Running uphill. Running on a hard surface. Quickly changing speeds from walking to running. Playing sports that cause you to quickly start and stop. Symptoms Often the person feels a whip-like blow that is followed by weakness in the affected leg - usually he or she is not able to walk afterwards. At place where the tendon ruptured, a significant dent is palpable. Often the experienced physician can diagnose a ruptured Achilles tendon by way of clinical examination and special function tests. Imaging techniques, such as ultrasound and magnetic resonance imaging (MRI) allow for a more precise diagnosis. Diagnosis Your doctor diagnoses the rupture based on symptoms, history of the injury and physical examination. Your doctor will gently squeeze the calf muscles, if the Achilles tendon is intact, there will be flexion movement of the foot, if it is ruptured, there will be no movement observed. Non Surgical Treatment Non-surgical treatment of Achilles tendon rupture is usually reserved for patients who are relatively sedentary or may be at higher risk for complications with surgical intervention (due to other associated medical problems). This involves a period of immobilization, followed by range of motion and strengthening exercises; unfortunately, it is associated with a higher risk of re-rupture of the tendon, and possibly a less optimal functional outcome.  Surgical Treatment Surgical correction of the ruptured tendon is almost always necessary. Surgery is performed in order to regain the maximum strength of the Achilles, as well as the normal pushing off strength of the foot. The strength of the muscle depends on the correct tension between the muscle and the tendon. The only way the correct tension on the tendon can set is by accurately repairing the tendon ends. When the tendon ruptures, the ends of the tendon separate and multiple little strands of the tendon are present like pieces of spaghetti. There are old fashioned techniques for repairing the tendon which require very long incisions (eight inches) on the back of the leg. These are complicated and associated with a high incidence of infection in the skin after surgery. This is an important consideration, since infection in the skin can lead to devastating problems with the skin and tendon. This problem of skin infection has, in the past, led surgeons away from surgical methods of treatment. Fortunately, now there is a new, unique method available for operating on and repairing the tendon. This new method requires only a tiny incision of one to two centimeters in length. This is far more accurate surgery. Recovery after this procedure is easier and the surgical complication rate is extremely low.
Surgical Treatment Surgical correction of the ruptured tendon is almost always necessary. Surgery is performed in order to regain the maximum strength of the Achilles, as well as the normal pushing off strength of the foot. The strength of the muscle depends on the correct tension between the muscle and the tendon. The only way the correct tension on the tendon can set is by accurately repairing the tendon ends. When the tendon ruptures, the ends of the tendon separate and multiple little strands of the tendon are present like pieces of spaghetti. There are old fashioned techniques for repairing the tendon which require very long incisions (eight inches) on the back of the leg. These are complicated and associated with a high incidence of infection in the skin after surgery. This is an important consideration, since infection in the skin can lead to devastating problems with the skin and tendon. This problem of skin infection has, in the past, led surgeons away from surgical methods of treatment. Fortunately, now there is a new, unique method available for operating on and repairing the tendon. This new method requires only a tiny incision of one to two centimeters in length. This is far more accurate surgery. Recovery after this procedure is easier and the surgical complication rate is extremely low.
The Achilles tendon is situated above the heel and forms the lower part of the calf muscles. It is a continuation of the two calf muscles, the gastrocnemius and soleus muscles, and it attaches to the heel bone. It is the strongest tendon in the human body and must withstand great forces. Its function is to transmit the force produced by the calf muscles to lift the heel and produce the push off during walking, running and jumping. The Achilles can produce force of up to seven times body weight. This shows just how much force it has to withstand during sporting activities, such as sprinting, jumping and turning. Causes The causes of an Achilles tendon rupture are very similar to Achilles tendinitis. Causes include. Running uphill. Running on a hard surface. Quickly changing speeds from walking to running. Playing sports that cause you to quickly start and stop. Symptoms Often the person feels a whip-like blow that is followed by weakness in the affected leg - usually he or she is not able to walk afterwards. At place where the tendon ruptured, a significant dent is palpable. Often the experienced physician can diagnose a ruptured Achilles tendon by way of clinical examination and special function tests. Imaging techniques, such as ultrasound and magnetic resonance imaging (MRI) allow for a more precise diagnosis. Diagnosis Your doctor diagnoses the rupture based on symptoms, history of the injury and physical examination. Your doctor will gently squeeze the calf muscles, if the Achilles tendon is intact, there will be flexion movement of the foot, if it is ruptured, there will be no movement observed. Non Surgical Treatment Non-surgical treatment of Achilles tendon rupture is usually reserved for patients who are relatively sedentary or may be at higher risk for complications with surgical intervention (due to other associated medical problems). This involves a period of immobilization, followed by range of motion and strengthening exercises; unfortunately, it is associated with a higher risk of re-rupture of the tendon, and possibly a less optimal functional outcome. Surgical Treatment Surgical correction of the ruptured tendon is almost always necessary. Surgery is performed in order to regain the maximum strength of the Achilles, as well as the normal pushing off strength of the foot. The strength of the muscle depends on the correct tension between the muscle and the tendon. The only way the correct tension on the tendon can set is by accurately repairing the tendon ends. When the tendon ruptures, the ends of the tendon separate and multiple little strands of the tendon are present like pieces of spaghetti. There are old fashioned techniques for repairing the tendon which require very long incisions (eight inches) on the back of the leg. These are complicated and associated with a high incidence of infection in the skin after surgery. This is an important consideration, since infection in the skin can lead to devastating problems with the skin and tendon. This problem of skin infection has, in the past, led surgeons away from surgical methods of treatment. Fortunately, now there is a new, unique method available for operating on and repairing the tendon. This new method requires only a tiny incision of one to two centimeters in length. This is far more accurate surgery. Recovery after this procedure is easier and the surgical complication rate is extremely low.
 Achilles tendinitis is an inflammation (swelling) of the tendon, which usually occurs as a result of overuse injury. Anyone can have Achilles tendonitis. Athletics involving frequent jumping is the classic cause, but certainly not the only one. Any activity requiring a constant pushing off the foot, such as running or dancing, may result in swelling of the tendon.
Achilles tendinitis is an inflammation (swelling) of the tendon, which usually occurs as a result of overuse injury. Anyone can have Achilles tendonitis. Athletics involving frequent jumping is the classic cause, but certainly not the only one. Any activity requiring a constant pushing off the foot, such as running or dancing, may result in swelling of the tendon.
 The Achilles tendon is the confluence of the independent tendons of the gastrocnemius and soleus, which fuse to become the Achilles tendon approximately 5 to 6 cm proximal to its insertion on the posterior surface of the calcaneus. The gastrocnemius and soleus muscles, via the Achilles tendon, function as the chief plantarflexors of the ankle joint. This musculotendinous unit provides the primary propulsive force for walking, running, and jumping. The normal Achilles tendon can withstand repetitive loads near its ultimate tensile strength, which approach 6 to 8 times body weight.
The Achilles tendon is the confluence of the independent tendons of the gastrocnemius and soleus, which fuse to become the Achilles tendon approximately 5 to 6 cm proximal to its insertion on the posterior surface of the calcaneus. The gastrocnemius and soleus muscles, via the Achilles tendon, function as the chief plantarflexors of the ankle joint. This musculotendinous unit provides the primary propulsive force for walking, running, and jumping. The normal Achilles tendon can withstand repetitive loads near its ultimate tensile strength, which approach 6 to 8 times body weight.
